
MEDICAL - GENERAL INFO
ANEMIA
Causes of enlarged red blood cells (aka macrocytic anemia):Vitamin B12 and Folic Acid tests: Two of the most common causes of enlarged red blood cells - that result in Macrocytic anemia, are low blood levels of vitamin B12 and folic acid.
A Schilling test: This urine test is done to help determine whether the body is absorbing B12 and the actual cause of why it may not be.
Homocysteine: Homocysteine is an amino acid normally found in minute amounts in the blood. A high blood level of homocysteine is a sign of B12 deficiency anemia.
Complete Blood Count (CBC): This blood test can easily spot problems with low levels of B12 by examining red blood cell count for anemia. It checks the red blood cells for shape, size, and quantity.
Methylmalonic acid (MMA) blood test: Methylmalonic acid is a substance in blood that increases when vitamin B12 levels decrease.
Be sure to ask your doctor for a copy of the lab results. Most labs will offer a normal and abnormal range value next to the result for reference. Having the results will help ease your mind and also can be reviewed against future lab results.
Low stomach acid, known as hypochlorhydria, interferes with the absorption of B12.
BACK PAIN
|
Intestinal Obstructions
|
A fat, bloated stomach on an otherwise thin person can be a sign of poor digestion. Controlled, enzymatic digestion is the normal way in which food is digested; when this is disrupted, putrification of the contents of the intestines is the result. The rotting products increase the likelihood of constipation. Often, one isn't aware of being constipated. There might be a bowel movement each day - but the contents might be eight days old instead of eight hours! This may be accompanied by foul smelling feces and wind. In such a case, a cure with apple vinegar can be helpful: 1 tablespoon in a glass of water, on an empty stomach, each morning. Colon hydrotherapy may also help.
From: www.weightlossresources.co.uk/diet/advice/bloating.htm
Constipation is one of the most common causes of bloating. If constipation is a problem, gradually increase the amount of fibre-rich foods you eat such as fruit, veg, wholegrain cereals. Drink up to eight glasses of water a day, as a lack of fluid can make constipation worse, especially if you're eating lots of fibre.
Some foods are also known to cause bloating: beans, broccoli, cauliflower, cabbage, sprouts, onions and garlic � however, remember these are good sources of fibre.
Swallowing too much air can also give you a bloated abdomen and there are several habits that can result in this: talking while eating, using a straw or sports bottle, chewing gum, eating when you're on the move, drinking from a water fountain and eating when you're upset are all common culprits so try and eliminate as many of these things as possible.
Some people blame bloating on an intolerance to a certain food such as wheat or dairy products. However, food intolerances are notoriously difficult to diagnose as the symptoms can be so wide ranging, including everything from bloating, fluid retention, headaches and tiredness to constipation and diarrhoea. If you really think you might have an intolerance I suggest you keep a food and symptoms diary to see if there's any pattern and then see your GP for a proper diagnosis.
Irritable bowel syndrome is also often associated with bloating. Usually a healthy diet will help you lose weight and keep the symptoms of IBS at bay.
Bloating is largely caused by intestinal gas. Intestinal gas can result from eating gassy foods or swallowing air. Swallowing air while eating is often done unconsciously and may result in frequent belching during or after meals. To avoid swallowing air, slow down when eating, don't 'slurp' drinks, and don't talk while chewing.
Foods that commonly cause gas are Asparagus, Broccoli, Brussels sprouts, Cabbage, Cauliflower, Corn, Fructose, Lactose, Potatoes, Sorbitol, Wheat.
Once the bloating is already present there are a few different ways to treat it. Activated charcoal in tablet form taken before and after meals may help reduce gas and bloating.
To expel intestinal gas try a brisk walk or other form of exercise. Frequent exercise can help keep the intestines moving properly. If exercise fails, try laying quietly on your left side and bring your knees up to your chest. This position can sometimes help release trapped gas.
Exhale all the air from your lungs hard while at the same time pulling your tummy in tight as if your belly button can touch your spine. Breathe lightly in this position and hold the posture for approximately 45 seconds. Repeat the exercise for 10 - 15 sets.
The second version involves doing the same exercise while on all fours in a crawling position. This adds gravity resistance. Do both exercises every other day. These exercises train your abs to continuously hold your stomach in, giving a flat appearance.When combined with a proper diet, weight training, and cardiovascular fitness you will get a flat stomach in a few weeks.
What are the symptoms?
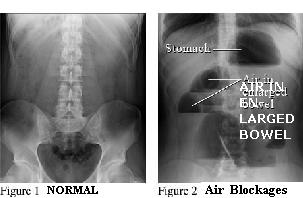
Crampy abdominal pain, vomiting, and bloating are the main symptoms of small-bowel obstruction. If blood supply is cut off (strangulation), the pain may be severe. Obstruction of the large intestine also causes abdominal pain and bloating. A partial intestinal blockage may cause occasional diarrhea. A complete obstruction will cause constipation and a noticeable lack of gas (flatus) leaving the body.
A bowel obstruction can be caused by twisting or narrowing of the intestines, tumors, or the formation of scar tissue (adhesions); these are called mechanical obstructions. Obstruction of the bowel can also occur when the intestines stop moving because of inflammation or infection or as a side effect of certain medications.
Mechanical obstructions in the small intestine are most frequently caused by scar tissue formation (adhesions). Other causes include hernias, Crohn's disease. In the large intestine, mechanical obstructions can be caused by tumors, twisting of the intestine or narrowing that may occur because of diverticulitis or inflammatory bowel disease, or one part of the intestine folding like a telescope into another part, which is called intussusception.
OTHER CONDITIONS with SIMILAR symptoms:
Inflammation of the pancreas (pancreatitis).
Inflammation of the gallbladder (acute cholecystitis).
DIAGNOSING AN OBSTRUCTION
Abdominal X-Ray - can detect blockages in the small and large intestines.
 |
| |
Barium Contrast X-Ray - not used as often as abdominal X-ray and CT scan to diagnose obstructions.
Ultrasound is increasingly being used to find obstructions in the small intestine.
A proctosigmoidoscopy may be done to find blockage in the large intestine, but only if the obstruction is partial and there is no sign of infection that could spread from a ruptured bowel (peritonitis). [Proctoscopy looks inside the anus, rectum, and the lower part of the large intestine (colon) for abnormal growths (such as tumors or polyps), inflammation, bleeding, hemorrhoids, and other conditions (such as diverticulosis). ]
If the proctosigmoidoscopy is normal, an X-ray using contrast material may be done to try to locate the obstruction.
Blood Tests
A complete blood count may also be done if an intestinal obstruction is possible. Strangulated obstruction is associated with a high white cell count. Electrolytes: Intestinal obstructions may result in low electrolyte levels, requiring treatment with mineral replacements. Creatinine and blood urea nitrogen, which measure how well the kidneys are working and whether a person is dehydrated.
How is a bowel obstruction treated?
Treatment for a partial blockage in the small or large intestine usually begins with close monitoring while waiting to see whether the blockage goes away on its own in the hospital. You are not allowed to eat or drink. Fluids are given intravenously to maintain hydration. A nasogastric (NG) tube may be placed in the nose and down into the stomach to remove fluids and gas; this may relieve pain and pressure.
These and other nonsurgical treatments are usually tried first for partial obstructions. Surgery is almost always needed for a complete obstruction of the small or large intestine or if blood supply is cut off (strangulation). Obstructions can recur if the underlying cause is not treated.
PSEUDO OBSTRUCTIONReasons for suspecting pseudo-obstruction include the feeling of standstill in the gastrointestinal tract, and severe episodes of distension (expansion of the abdomen). Disease mainly affecting the large bowel may manifest as severe constipation. Most cases involve pain, cramps, & sometimes malnutrition. Like most gastrointestinal diseases, pseudo-obstruction cannot be recognised from the outside of the patient. Blood tests are usually normal and even an extensive investigation including ultrasonography, computed tomography, gastroscopy, barium meal, barium enema and colonoscopy may yield normal results. Dilated bowel loops can be seen in some patients, usually with advanced myopathic pseudo-obstruction.
Difficult to Diagnose:
Different types of pseudo-obstruction: Another type is caused by damage to the muscles of the bowel wall. Damage to the muscle cells is called visceral myopathy and leads to myopathic pseudo-obstruction. Visceral ["primal"] myopathy [muscle disorder] causes weakening of the muscular contractions. Sometimes visceral myopathy can present as long-standing cramps in the muscles of the gut.
Treatment:
|
 |
| A basic elastic knee brace helps prevent the kneecap from dislocating. |
Dislocated Kneecap: An injury, ligament damage, or simply the way your bones fit together can cause the kneecap to dislocate (slip out of place). It may slip only once. Or it may slip many times without warning. You may feel sudden, sharp pain, or your knee may "give out."

|
|
|
Q: My kneecap keeps dislocating. What can be done about this?
A: If a kneecap (patella) keeps dislocating, there is generally an anatomical problem preventing proper alignment and tracking of the kneecap as the knee bends and straightens. This may be due to faulty development of the kneecap itself, faulty development of the condyles of the femur, over which the kneecap slides, or over tight lateral structures or over weak medial structures. Operations (in order of magnitude) may include lateral release or medial reefing (which concentrate on the medial and lateral structures), Roux-Goldthwaite or Elmsley-Trillat procedures (which concentrate on re-aligning the patellar tendon) and finally trochleoplasty (which re-shapes the groove in which the kneecap tracks.
-------
[http://forums.ebay.co.uk/thread.jsp?forum=1003&thread=300002892&modifed=20040114192824 ]
Hi, has anybody had keyhole surgery on the knee for cartilage problems?
Mine keeps just locking, and then will not hold me. Damn painful. Your daughter has my every sympathy.
When my brother had it for a rugby injury, I think he had to convalesce for three weeks, but the operation itself was done in an afternoon at out-patients
It has happened three times now. The cartilage is unstable and her knee just pops out. Last time it didn't
go back
Hi
I am probably too late to answer this now.
I have had keyhole surgery on my knee twice.
Th first time was about 5 years ago, day patient, stitched the entry wound, 2 very tiny scars, very little pain but on crutches for about 1 week.
-------------
www.vandemarkortho.com/patient/pated/knee_problems/patella/knee_patella.html
Looking at the end view of the knee shows how loosening these ligaments may relieve pressure on the articular cartilage. Once the ligaments are cut, the patella moves more into the center of the femoral groove, and tracks more in the center of the groove. In some cases of severe malalignment, a lateral release alone may not be enough. If the malalignment is so bad that the patella (Kneecap) dislocates repeatedly, then the operation will have to include a more involved realignment of the quadriceps mechanism. In addition to the lateral release, the tendons on the inside edge of the knee (the medial side) may have to be tightened as well. In very severe cases of malalignment, the attachment of the patellar tendon may also have to be moved.
------------
[http://www.americanrunning.org/displayindustryarticle.cfm?articlenbr=1700 ]
Dislocated Patella (Kneecap)
Your patella (kneecap) is shaped like a disc and sits at the end of femur (thigh bone). When your knee is bent, it rides in a groove at the end of your thigh bone. Two types of dislocations can occur: complete or subluxing. Complete occurs when your kneecap becomes totally dislocated and won't sit in the groove.
Subluxing occurs when your kneecap slips out of the groove slightly, causing pain but not limited motion. When either of these scenarios occur, parts of the kneecap can fracture. The fragments of cartilage and bone can become loose and create mechanical problems in the joint.
Signs and Symptoms:
If your dislocation is complete, you won't be able to straighten out your knee without experiencing some pain. If it's subluxing, you'll feel pain when you climb stairs, and when you arise from a seated position or squat. You'll also have the anxious feeling that your kneecap is going to shift out of place.
Causes:
1. Twisting. You normally dislocate your patella while doing some twisting activity like swinging a bat , or quickly changing direction.
2. Direct Trauma. Your patella can become dislocated by a hard blow, like you may experience while playing football or another contact sport.
3. Muscle Imbalance. Often, one of your quadriceps muscles (Vastus Medialis) is weaker than another (Vastus Lateralis). The stronger outside quadriceps (vastus lateralis) contracts, it pulls the patella to the outside, leading to a dislocated patella.
RX Measures:
With an acute dislocation of the kneecap, the knee must be straightened out and the kneecap can usually, fairly easily, be pushed back into place. The knee must then be immobilized for four to six weeks followed be an aggressive rehabilitation program.
See your physician if your patella is completely out of place. It may require reduction under an anesthetic. You'll need to wear a brace for several weeks. Your doctor will determine at this time whether any further damage has been done. If it has, or if it becomes recurrent or there are mechanical problems, arthroscopic surgery may be discussed.
To Avoid Future Problems: Quadriceps strengthening exercises are strongly recommended. If you have a chronic subluxing dislocation, aim to keep all of your quadriceps muscles strong, especially the Vastus Medialis muscle. Leg extensions must be performed in the final 30-degrees of extension, for this is when this muscle is most activated. You should talk to your physical therapist about this. In addition hamstring and iliotibial band flexibility is imperative.
Surgery. In cases of chronic dislocations, surgery to realign the kneecap may be needed. However, the need for surgery is relatively rare.
Safe Alternative Training: Any activity with the knee in full extension will usually not cause great discomfort and can be considered safe. This could include isometrics of the quadriceps muscle, straight leg raising exercises, etc.
--------
The gallbladder is a small pear shaped organ under the liver in the upper right side of the abdominal cavity. It collects and concentrates bile, which the body uses to digest fats. Some gallbladder problems include:
http://www.csmc.edu/5688.html
Kidney stones develop when the urine is supersaturated with salts that can form into stones. This includes overexcretion of salt, having acid urine or having a low volume of urine. The primary risk factor for kidney stones is family history.
Kidney stones can develop as a result of:
At the very beginning of kidney stone pain, begin drinking lukewarm water. Drink as much as you comfortably can, as quickly as you can, one or two pints minimum in the first 10 minutes. Put on a pair of shoes sturdy enough for jumping in. Decide what hard surface area, such as garage or basement floor, you will use.
After about 25 - 30 minutes from the time you began to drink the lukewarm water, you are ready for step number two. You may experience some increase in pain during the 25 - 30 minutes of prep period; however, this should be assurance that you have developed a nice, heavy, jet of urine that will quickly (within 15 - 25 minutes) move your stone to the bladder. In fact, if you do not experience some small increase in pain, it could mean that a small stone (3-4 mm or less) is involved, creating only partial obstruction. This results in a small, lightweight, liquid tool, in which case it could take as much as 40 � 50 minutes to move the stone to the bladder.
Step Two:
Now you are ready for the "exercise". Jump vertically, at least an inch or two, and land as stiffly as possible, with the ankles, knees, and hips "locked." Immediately repeat the jump,
Wait about 5 minutes and do another pair of jumps.
Wait about 5 minutes and do another pair of jumps.
Wait about 5 minutes and do another pair of jumps.
Continue this pattern for about 45 � 50 minutes, or until complete cessation of pain, whichever comes first.
After about 5 to 10 minutes from the first pair of jumps, empty the bladder, and continue to do so about every 10 minutes thereafter. There is a good reason for keeping the bladder nearly empty during the procedure. The literature clearly shows that there is less resistance by the bladder to the transfer of urine from the ureter to the bladder when the bladder is empty than when it is full, or partially full. Therefore, we can assume that this might also be true for a stone. It makes sense that a stone will go into the bladder more easily when the bladder is empty, or nearly empty, than when it is full or partially full.
All of the basic instructions for the jump method apply to the bump method. With the bump method, the bumping site might be different than the jumping site. An open toilet seat should be ideal for most individuals. The main reason is that no special arrangements need to be made to protect the genitals from damage, as would be required on a hard flat surface. As for males, since the testicles can be pulled upward by a jock strap or by hand, toward the navel, most any hard, flat surface of suitable height is fine.
Beginning the actual BUMP procedure:
Back up to the toilet seat - or other hard flat surface - as if to sit down. But instead of sitting completely down:
"Magnesium is essential: it acidifies the urine and stones cannot be formed in acid urine. Vit B6 prevents the formation of oxalic acid kidney stones. Also take calcium: if calcium is lacking, the body will withdraw it from the bones and form the stones just the same. As magnesium interacts with calcium, if taken in the right proportions (300 mgs of magnesium per 1 gram of calcium), kidney stones are not formed and/or can be dissolved."
2 0z. Lemon Juice w/ 2 oz. Olive Oil - Holistic Remedies
Low water intake can cause a deficient flow of nutrients to parts of the body. Hydration of muscles is essential to avoid cramping during sleep or after exercise.
Another cause of leg cramps is mineral deficiencies: low levels of salt, calcium, potassium and magnesium in the body. Calcium deficiency causes muscle tremors and twitching which further leads to leg cramps. Potassium and magnesium help in controlling muscles and maintain body fluid balance. Deficiency of these two minerals can lead to painful, sudden leg cramps.
Some other factors that contribute to this condition are:
When you get a cramp, walk on the affected leg and then elevate it. Stretch your calf by grabbing your toes and pulling them upward toward your knee, with you leg extended straight.
The natural way to eliminate cramping in your muscles is to watch out for limited salt consumption. If you've been sweating - but neglecting your salt & water intake, this is the likely culprit.
This causes the release of chemicals from nerve fibers that coil around the large arteries of the brain. This stretches the nerves and causes them to release chemicals. The chemicals cause inflammation, pain, and further enlargement of the artery. The increasing enlargement of the arteries magnifies the pain.
Migraine attacks commonly activate the sympathetic nervous system in the body. The sympathetic nervous system is the part of the nervous system that controls primitive responses to stress and pain, the so-called "fight or flight" response, and this activation can cause other symptoms related to fight-or-flight nervous stimuli.
Migraine headaches that are associated with episodes of vertigo are known as vestibular migraines. The term �vestibular� refers to the inner ear where we sense balance. Vestibular migraines are not the most common type of headache, but they can be quite debilitating.
Episodes of vertigo could last for minutes to an hour before a migraine starts. Some people who have vestibular migraines will also see changes in their vision like bright or flashing lights, or spots in their line of sight. They will also have many of the more common migraine symptoms, like photophobia, phonophobia, severe throbbing head pain, nausea, or vomiting.
Vestibular migraines are treated the same way as �normal� migraine headaches,
Triggers:
More from: http://www.underworks.com/health/419.html
If you are bitten or scratched by an animal that you think may have rabies, you should:
1. Wash the wound well with soap and warm water for at least five minutes. This lessens the chance of any infection.
2. Seek medical attention right away.
If treated in time, rabies in humans can be prevented.
If you require treatment, two products are used:
Rabies immune globulin; and Rabies vaccine.
If you will be travelling for a month or more to areas where rabies is often found in a number of different animals, consider being vaccinated for rabies before you go.
More: www.bchealthguide.org/healthfiles/hfile07.stm
|
[ www.clevelandclinic.org/health/health-info/docs/1700/1707.asp?index=7079&src=news ]
Symptoms include difficulty reaching up behind the back, pain with overhead use of the arm and weakness of shoulder muscles. Aspirin, naproxen / ibuprofen remain the most common treatment. A patient must consistently take the medication for eight weeks to effectively treat their condition. Daily stretching in a warm shower will help. Patients should work to reach their thumb up and behind their back. Finally, the patient should avoid repetitive activities with their injured arm, particularly where the elbow would move above shoulder level. Activities such as vacuuming, painting, raking leaves and washing a car should be avoided to minimize the use of the sore muscle. |
2. Frozen Shoulder is slightly different from Impingement Syndrome. It's a severely restrictive condition in which the shoulder capsule contracts or becomes inflamed, causing adhesions and scaring that "freeze" the shoulder. Intermittent use may cause this. There is also a lack of synovial fluid to lubricate the gap between the arm bone and socket that normally helps the shoulder joint to move.
Frozen shoulder causes a dull, vague pain over the deltoid region that worsens with movement and at night when lying on the shoulder. It's difficult to put on or remove a t-shirt, reach for a wallet in a back pocket, or comb his/her hair. Usually the person experiences a gradual onset of pain rather than sudden injury. People with frozen shoulder often have a rounded-shoulder posture The involved arm is held in a hiked position close to the body. Movement is limited in external rotation (rotation outward), and limited in lifting the arm up and outward, and internal rotation. Treatment: There are three stages of frozen shoulder. The first stage (the "painful stage") involves inflammation, pain at rest, and inability to move shoulder in all directions. This is treated with rest, gentle exercises (i.e. pendulums), anti-inflammatories (i.e., asprin) and pain medication, and ice/heat treatment. The second stage is the frozen or stiff phase. Intermittent pain and stiffness limits movement in the shoulder. Pain occurs when the arm moves to the limit of range. This stage can last 4-12 months. A program of self stretching exercises prescribed by a physical therapist may help shorten the period of limitation. And the third and final stage is the thawing phase. Shoulder stiffness is the main problem. Treatment includes: soft tissue massage, joint movement; and, therapeutic exercises. This can take up to two years. The entire duration from onset to recovery averages 30 months. [NOTE: The "Rotator Cuff Exercises," below, are also prescribed for "frozen shoulder" (gently, according to the "stage" of healing).] |
|
| |||
| |||
|
 |  |
| SIDE LIFT (right) with light weight. |
| ||
|
| ||
|
...is used to restore flexibility to the shoulder joint. It also relieves pressure on the rotator cuff. The exercise is performed as follows:
Relax your shoulder muscles.
While standing or sitting, keep your arm vertical and close to your body (bending over too far may pinch the rotator cuff tendons). Allow your arm to swing back and forth or in a small diameter circle no greater than 1 inch in any direction. Initially perform the exercise with just the weight of your arm. As pain subsides, hold a 5- to 10-pound weight in your hand (a filled gallon container weighs 8 pounds). Perform exercise for five minutes once or twice a day.
 |  |
IMAGES (Google) for Frozen Shoulder
[More Exercises on: http://www.public.iastate.edu/~jnespor/injury.html ]
Low back pain and/or leg pain that usually travels down the large sciatic nerve, from the lower back down the back of each leg, is generally referred to as sciatica and is fairly common. It is usually caused by pressure on the sciatic nerve from a herniated disc in the lumbar spine.
Often a particular event or injury does not cause sciatica, but rather it may develop as a result of general wear and tear on the structures of the lower spine. The vast majority of people who experience sciatica get better with time (usually a few weeks or months) and find pain relief with non-surgical treatments.
Usually, sciatica only affects one side of the lower body, and the pain often radiates from the lower back all the way through the back of the thigh and down through the leg. Low back pain may be present along with the leg pain, but usually the low back pain is less severe than the leg pain.
Possible causes:
The sciatic nerve may be harmed by pressure from masses such as a tumor or abscess, or by bleeding in the pelvis.
The veins however, work in a different way than the arteries. The blood is pushed through the arteries by the pump action of the heart, and are regulated by the restricting and dilating of the smooth muscle around the arteries. The veins don`t have as much smooth muscle, and they work differently.
The blood returning to the heart is being pushed up mainly by the Venous Plexus in the soul of the feet, and by the calf muscles.
Massaging the leg from ankle to leg improves the circulation by manipulation with the blood flow.
Start at the ankle: place your palms on each side of the leg. Using your thumb, firmly press down and push in a straight line all the way up to the knee. You will feel the bone in between your thumbs on the way up. Now go back down to the ankle, spread your thumbs a little farther apart and repeat the pressured straight line up to the knee. If you are able to reach around and do this to the back of the leg, repeat the pressured line.
Step 2. Firmly hold the ankle with one hand and place the other hand with the four fingers (not the thumb) on the calf muscle. Begin rotating deep,circular motions into the calf. Continue as long as desired.
 www.tchain.com/otoneurology/disorders/bppv/bppv.html
www.tchain.com/otoneurology/disorders/bppv/bppv.html
In Benign Paroxysmal Positional Vertigo (BPPV) dizziness is thought to be due to debris which has collected within a part of the inner ear. This debris can be thought of as "ear rocks", although the formal name is "otoconia". Ear rocks are small crystals of calcium carbonate derived from a structure in the ear called the "utricle".
BPPV is a common cause of dizziness. The symptoms of BPPV include dizziness or vertigo, lightheadedness, imbalance, and nausea. symptoms are almost always precipitated by a change of position of the head with respect to gravity. Getting out of bed or rolling over in bed are common "problem" motions . Because people with BPPV often feel dizzy and unsteady when they tip their heads back to look up, sometimes BPPV is called "top shelf vertigo." An intermittent pattern is common. BPPV may be present for a few weeks, then stop, then come back again.
The most common cause of BPPV in people under age 50 is head injury . In older people, the most common cause is degeneration of the vestibular system of the inner ear. In half of all cases, BPPV is called "idiopathic," which means it occurs for no known reason.
BPPV has often been described as "self-limiting" because symptoms often subside or disappear within six months of onset. Symptoms tend to wax and wane. Motion sickness medications are sometimes helpful in controlling the nausea associated with BPPV but are otherwise rarely beneficial. However, various kinds of physical maneuvers and exercises have proved effective.
The Epley maneuver is also called the particle repositioning, canalith repositioning procedure, and modified liberatory maneuver. It is illustrated in figure 2. It involves sequential movement of the head into four positions, staying in each position for roughly 30 seconds. The recurrence rate for BPPV after these maneuvers is about 30 percent at one year, and in some instances a second treatment may be necessary.
While some authors advocate use of vibration in the Epley maneuver, we have not found this useful in a study of our patients (Hain et al, 2000). Some authors also suggest leaving out some of the positions in the Epley maneuver, especially position 'D'. We suggest that you avoid therapy using this methodology. After either of these maneuvers, you should be prepared to follow the instructions below, which are aimed at reducing the chance that debris might fall back into the sensitive back part of the ear.
 1. Wait for 10 minutes after the maneuver is performed before going home. This is to avoid "quick spins," or brief bursts of vertigo as debris repositions itself immediately after the maneuver. Don't drive yourself home.
1. Wait for 10 minutes after the maneuver is performed before going home. This is to avoid "quick spins," or brief bursts of vertigo as debris repositions itself immediately after the maneuver. Don't drive yourself home.
2. Sleep semi-recumbent for the next two nights. This means sleep with your head halfway between being flat and upright (a 45 degree angle). This is most easily done by using a recliner chair or by using pillows arranged on a couch (see figure 3). During the day, try to keep your head vertical. You must not go to the hairdresser or dentist. No exercise which requires head movement. When men shave under their chins, they should bend their bodies forward in order to keep their head vertical. If eyedrops are required, try to put them in without tilting the head back. Shampoo only under the shower.
3. For at least one week, avoid provoking head positions that might bring BPPV on again.
Use two pillows when you sleep. /
Avoid sleeping on the "bad" side. /
Don't turn your head far up or far down. /
Be careful to avoid head-extended position, in which you are lying on your back, especially with your head turned towards the affected side. This means be cautious at the beauty parlor, dentist's office, and while undergoing minor surgery. Try to stay as upright as possible. Exercises for low-back pain should be stopped for a week. No "sit-ups" should be done for at least one week and no "crawl" swimming. (Breast stroke is OK.) Also avoid far head-forward positions such as might occur in certain exercises (i.e. touching the toes). Do not start doing the Brandt-Daroff exercises immediately or 2 days after the Epley maneuver, unless specifically instructed otherwise by your health care provider.
4. At one week after treatment, put yourself in the position that usually makes you dizzy. Position yourself cautiously and under conditions in which you can't fall or hurt yourself. Let your doctor know how you did.
Comment: Massoud and Ireland (1996) stated that post-treatment instructions were not necessary. While we respect these authors, at this writing (2002), we still feel it best to follow the procedure recommended by Epley.
 The Brandt-Daroff Exercises are a method of treating BPPV, usually used when the office treatment fails. They succeed in 95% of cases but are more arduous than the office treatments. These exercises are performed in three sets per day for two weeks. In each set, one performs the maneuver as shown five times.
The Brandt-Daroff Exercises are a method of treating BPPV, usually used when the office treatment fails. They succeed in 95% of cases but are more arduous than the office treatments. These exercises are performed in three sets per day for two weeks. In each set, one performs the maneuver as shown five times.
1 repetition = maneuver done to each side in turn (takes 2 minutes). Suggested Duration for the Brandt-Daroff exercises is 5 REPITITIONS, 2 MINUTES EACH (For a total of 10 MINUTES), 3 times a day - morning, noon, night. Start sitting upright (position 1). Then move into the side-lying position (position 2), with the head angled upward about halfway. An easy way to remember this is to imagine someone standing about 6 feet in front of you, and just keep looking at their head at all times. Stay in the side-lying position for 30 seconds, or until the dizziness subsides if this is longer, then go back to the sitting position (position 3).
Stay there for 30 seconds, and then go to the opposite side (position 4) and follow the same routine. These exercises should be performed for two weeks, three times per day, or for three weeks, twice per day. This adds up to 52 sets in total. In most persons, complete relief from symptoms is obtained after 30 sets, or about 10 days. In approximately 30 percent of patients, BPPV will recur within one year. If BPPV recurs, you may wish to add one 10-minute exercise to your daily routine (Amin et al, 1999). The Brandt-Daroff exercises as well as the Semont and Epley maneuvers are compared in an article by Brandt (1994), listed in the reference section.
----------------
For at least one week, avoid provoking head positions that might bring BPPV on again.
Use two pillows when you sleep. /
Avoid sleeping on the "bad" side. /
Don't turn your head far up or far down. /
Be careful to avoid head-extended position, in which you are lying on your back, especially with your head turned towards the affected side. This means be cautious at the beauty parlor, dentist's office, and while undergoing minor surgery. Try to stay as upright as possible. Exercises for low-back pain should be stopped for a week. No "sit-ups" should be done for at least one week and no "crawl" swimming. (Breast stroke is OK.) Also avoid far head-forward positions such as might occur in certain exercises (i.e. touching the toes). Do not start doing the Brandt-Daroff exercises immediately or 2 days after the Epley or Semont maneuver, unless specifically instructed otherwise by your health care provider.
Men's Health Forum Messageboard






